FNA vs. Core
FNA BIOPSY

Fine Needle Aspiration biopsy (FNA) uses a very thin needle attached to a syringe to withdraw (aspirate) a sample from a mass that can be felt (palpated) or a mass that can be visualized by ultrasound. The FNA sample consists of small tissue fragments and individual cells. The sample (tissue) is spread on a glass microscope slide, stained and looked at under the microscope. The needles used for FNA biopsy are typically smaller than needles used to draw blood. The needles are so thin that a local injectable anesthetic is usually not used. At OCC we use a topical lidocaine gel or ethyl chloride spray prior to the biopsy for patient comfort. FNA biopsies can usually be done, even if the patient is taking an anticoagulant. Most masses are sampled 3 to 4 times for an FNA biopsy to allow for adequate sampling.
CORE BIOPSY

Core needle biopsy (CNB) uses a thicker (larger gauge) needle so that small cylinders of visible tissue are procured. The sample must be fixed in formalin, processed overnight, embedded in paraffin, cut into thin sections with a microtome and then stained before a pathologist can look at the specimen under the microscope. Due to the larger size of the needle, an injectable anesthetic is usually administered; patients need to be off of their anticoagulant medications. For adequate sampling, 5-8 core biopsies of a mass are common.
FNA vs. Core sample volume
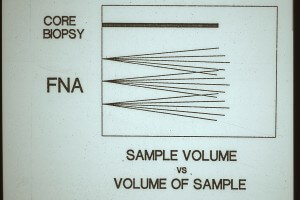
Amazingly, the volume of tumor cells sampled by FNA biopsy is greater than by CNB. The FNA needle can be safely moved through the suspicious mass for sampling whereas the CNB can only sample one area.
Since tumor cells tend to be loosely cohesive, they can be easily extracted from a mass with FNA and the surrounding fibrous tissue and stroma are not removed. In a CNB there is a mixture of tumor cells and non-diagnostic fibrous tissue and stroma.